Evidence & Research
Please note that in some instances you may not be able to access the journal article on line. If you have any difficulties please contact us for a copy.
Gaillard, A. S., Braun, E., Vollmann, J., Gather, J., & Scholten, M. (2023). The Content of Psychiatric Advance Directives: A Systematic Review. Psychiatric services (Washington, D.C.), 74(1), 44–55. https://doi.org/10.1176/appi.ps.202200002
This document is an international review of Advanced Health Directives. It gives a really good overview about current practices. Notice how service users are generally positive about Advanced Health Directives, while clinical staff are less so. One of the issues internationally and in Australia is the poor uptake of Advanced Health Directives.
The theme related to coercion in mental health care is particularly important to note – see page 51. Gaillard and colleagues report that: “Service users in 21 (50%) of the studies included in their PADs information on de-escalation and coping strategies to prevent or reduce the use of coercive measures as well as preferences regarding coercive measures themselves—should they be inevitable—or endorsed the inclusion of these preferences hypothetically.”
In two of the hypothetical studies, the inclusion of de-escalation strategies was endorsed by high majorities: 22 (96%) of 23 service users in one study and 91 (83%) of 110 service users in the other.
Gilliard et al. continue, “these strategies included reaching out to and connecting with others, involving mental health professionals, being left alone, and help in the management of emotions. In this context, one service user explained, “I don’t want threats of an injection; I would like people to talk to me explaining the need to take medication”. Others requested changes in medication or additional medication as de-escalation strategies. […] Service users also refused or requested specific coercive measures such as physical restraint and seclusion because of previous negative experiences with these or other measures. […] Service users in two studies provided a ranking from most to least preferred coercive intervention chosen from a specified list in one of the studies, whereby medication in pill form was most preferred, and seclusion plus restraint was least preferred. These preferences were often backed up by plausible reasons.”
This research shows how considered the responses are in how people complete an Advanced Health Directive. The responses are measured, relevant and informed by previous experiences and the person’s desire to avoid harmful practices.
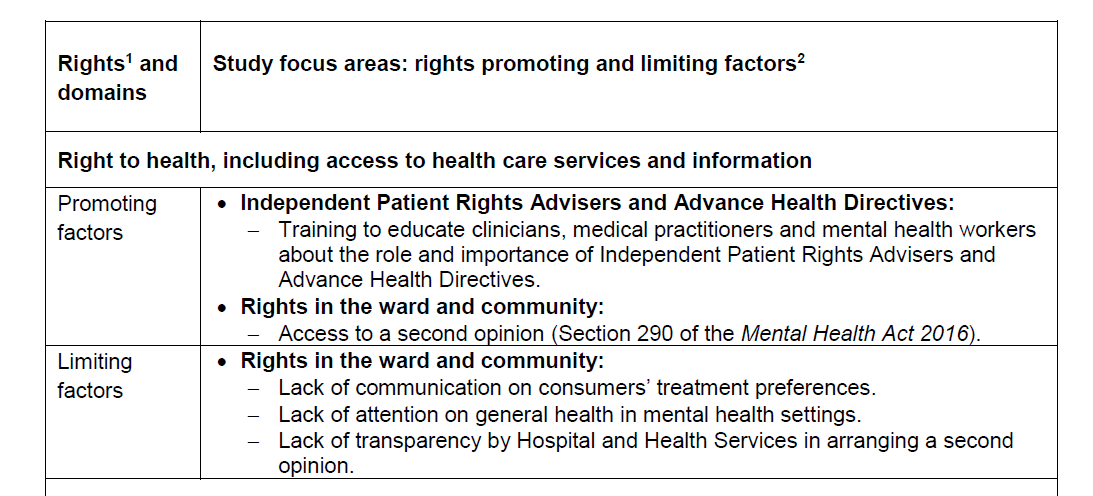
Queensland Mental Health Commission (2019). Human rights protection frameworks for people being treated involuntarily for mental illness: Overview. Queensland Government.
Scroll to the bottom of the page for a pdf copy of the Overview.
Research participants provided their views on mental patients’ rights and information – pages 9 to 10 are worth reading for the details behind the summary table below. Also, specifically in relation to Advanced Health Directives, read pages 11 to 12. Note how for one participant gaining support from an Independent Patients’ Rights Advisor was helpful in completing the form.
The diagram on p. 19 of the Overview summarises some key points from the research undertaken:
Another government report is very pertinent as it focuses solely on seclusion and restraint.
Gibson, N., et al. (2023). Mental Health Act 2016 report: Review of the use of seclusion and restraint. Queensland Government. https://www.health.qld.gov.au/__data/assets/pdf_file/0030/1287642/The-Mental-Health-Act-2016-Report.pdf
This review found similar concerns to other reports and research about the harmful impacts of seclusion and restraint. It also confirmed the pivotal role of the State’s chief Psychiatrist in leading reforms to eliminate the use of seclusion and restraint. An example of the focus areas is provided by the excerpt below from pages 6 to 7:
“Reviewing the regulatory framework to consider whether amendments are required to the framework to capture different population needs more appropriately, such as the needs of young people, high risk consumers and consumers on forensic order (disability).
And
Undertaking a project to evaluate the use of seclusion and restraint forms within operational and clinical practice, to identify opportunities to reduce administrative reporting requirements that do not support the protection of patients’ rights, reflect contemporary clinical practice or support efforts to reduce the use of seclusion and restraint. This project should be undertaken in collaboration with services and be supported by evidence around a common goal; use standards, processes, policies and infrastructure to enable multi-actor collaboration; and … create and share resources to achieve goals.”
Meanwhile, the Queensland Government’s response to the review of the Mental Health Act can be found here.
On reading this document it can be hard to discern if any significant change is imminent in the short term to the use of seclusion and restraint in mental health facilities. The Government continues to state that it is committed to the reduction and elimination of these restrictive practices. While in actuality they continue allow their use, knowing they are harmful. The knowledge and changes to clinical practices needed are already known. A review by the NSW Government after the death of a patient who had been secluded, details the need for mental health system wide changes and workplace support and development. This details about the NSW report are provided below:
Wright, M. (2017). Review of seclusion, restraint and observation of consumers with a mental illness in NSW Health facilities. NSW Government. https://www.health.nsw.gov.au/mentalhealth/reviews/seclusionprevention/Documents/report-seclusion-restraint-observation.pdf
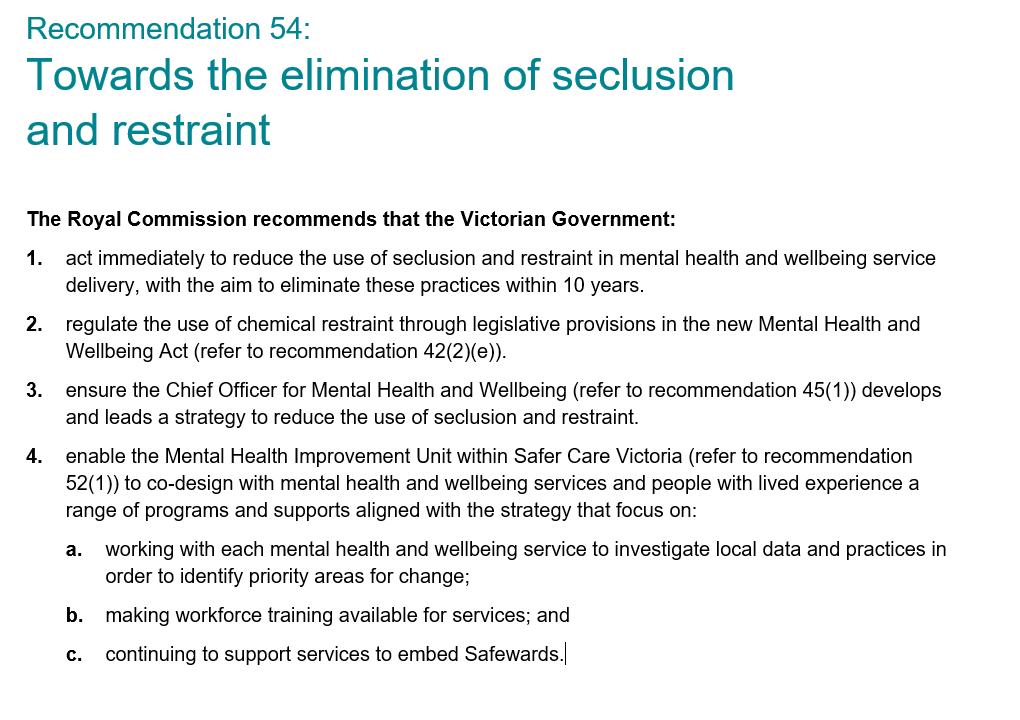
The report is overshadowed by more recent government inquiries such as the Victorian Royal Commission into Victoria’s mental health services. https://www.vic.gov.au/royal-commission-victorias-mental-health-system-final-report
The final report, which was handed to the State Government in 2021, has a broad range of recommendations, similar to the NSW report by Wright (2017). The most pertinent points are on page 91 where the Royal Commissioners summarise their recommendations with regard to seclusion and restraint
The personal testimonies of witnesses are devastating for the harm and trauma they experienced while in a mental health facility. There is little evidence of improved safety and wellbeing of patients in state government mental health facilities as a result of these reports and recommendations.
Many of the reports can be hard to read due to the amount of material and there can seem to be no answers for people wanting to be heard and keep safe if they are hospitalised. Some of the most useful resources are found in documents that centre on the experiences of people with lived experience. As just one example is this one that was created by Victorian Legal Aid as part of the public submissions to the Victorian Royal Commission, which can be found here.
On page 4, there is a summary table of the views of people with lived experience
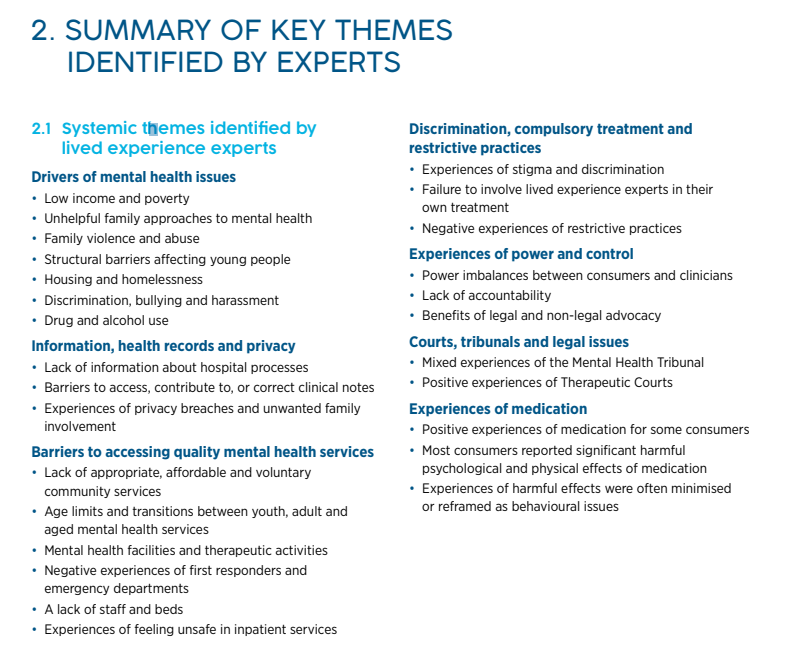
This mirrors other Australian research by the following researchers:
Brophy, L., Roper, C., Hamilton, B., Tellez, J., & McSherry, B. (2016). Consumers’ and their supporters’ perspectives on barriers and strategies to reducing seclusion and restraint in mental health settings. Australian Health Review, 40(6), 599–604. doi:10.1071/AH15128
The abstract follows:
Objective: This paper examines the perspectives of consumers and their supporters regarding the use of seclusion and restraint in mental health settings.
Methods: Five focus groups for consumers and five focus groups for supporters were conducted in four Australian cities and in one rural location. The 66 participants were asked about strategies to reduce or eliminate the use of seclusion and restraint in mental health settings.
Results: All participants supported the reduction of the use of seclusion and restraint. Barriers to reducing these practices related to the environment, the effects of drug and alcohol issues, lack of a human rights focus and poor recognition of trauma, stigma and discrimination. Strategies for reducing or eliminating seclusion and restraint included workforce development, environmental and cultural changes.
Conclusions: Participants clearly identified that the status quo needs to change and conveyed urgency for action. Participants suggested that the involvement of supporters and a range of consumer roles are integral to reducing the use of seclusion and restraint. The findings support the current policy emphasis of working towards the elimination of these practices. What is known about the topic? Mental health policies across many jurisdictions support the reduction and elimination of restraint and seclusion. Evidence suggests those subjected to restraint and seclusion largely experience a range of harmful consequences. No studies focus on the views of supporters of consumers regarding the reduction and elimination of seclusion and restraint, whereas the views of consumers appear in a minority of international studies.
What does this paper add? The research enabled an opportunity to hear from people who have been personally affected by and/or have lived experience of these coercive practices. Participants identified local reforms that can uphold the human rights of consumers. They suggested practices to increase accountability, peer support and family involvement, areas that have not been analysed in depth in any of the seclusion and restraint literature. What are the implications for practitioners? This paper will give healthcare services a deeper insight into how to reduce or eliminate restraint or seclusion from the perspective of those with lived experience.
Finally, two publications by a member of the research team who put this web page together provide the main understandings we were informed by at the outset of the project. These ideas have subsequently been strongly augmented by the views of people with a lived experience of mental health, some of whom have created videos for this page.
Ross, D. (2020). ‘Towards coercion free, trauma-informed care in Australian adult mental health services: Strategies for social workers’. Social Work and Mental Health. 18: 5, pp. 536-553. DOI 10.1080/15332985.2020.1801552
The abstract follows:
Least restrictive practice is a key principle of mental health legislation. It seeks to minimize coercion and maximize the human rights of mental health service users. Coercive practice, with a focus on seclusion, is explored from a whole-of-mental-health-system perspective as distinct from the behavior of individual service users. Exemplar coercion-reducing strategies arising from the reviewed research and literature are outlined. The exemplars can strengthen the utility of the least restrictive principle by extending non-coercive practice options for mental health social workers. The strategies bring a focus to proactive trauma-informed systemic changes and community level alternatives to hospitalization, coercion and seclusion.
Ross, D. (2018). ‘A social work perspective on seclusion and restraint in Australia’s public mental health system’, Journal of Progressive Human Services: Radical Thought and Praxis. 29: 1, pp. 1-19. DOI: 10.1080/10428232.2018.1442972
The abstract for the second article follows:
A social work perspective of the nature of seclusion and restraint in Australia’s public mental health systems is presented. The article suggests a theme of seclusion and restraint as a regulatory mechanism despite evidence of harm and even death. The case that the use of seclusion and restraint constitutes a social justice issue as it can be understood as an abuse of human rights and form of torture is established. An incident of a person dying in an Australian mental health facility after being secluded is presented to substantiate this claim. An over focus on individual expressions of violence or risk can be at the expense of understanding the systemic and cultural nature of violence in mental health systems. It is important to understand the nature of, and perhaps to question the presumed necessity of, seclusion and restraint practices to ensure that social workers are not breaching their professional obligations to people who are mental health clients.
Final comment:
What might all this mean for you or someone you know if you/they are a patient in a mental health facility?
It is most important that you/the person you know are the best possible self advocates. To feel safe and be heard will need you to act to remain empowered. Advanced Health Directives have been shown to work, if used and if placed in the hands of the treating team and your support people.